Abdominal Wall Reconstruction & Abdominoplasty/Panniculectomy
What is a hernia?
Hernia is the general term used to describe the phenomena when an organ or other bodily structure protrudes through the wall that normally contains it. This is most frequently applied to the herniation of abdominal organs (most likely the small intestines) through the abdominal fascia. A ventral hernia, a specific type of hernia, involves the protrusion of organ tissue through the midline of the abdominal wall. Depending on the severity of the herniation a general surgeon may choose to work with a plastic surgeon to reconstruct the defect responsible for the hernia. Abdominal wall reconstruction is commonly combined with an abdominoplasty and/or panniculectomy.
Candidates:
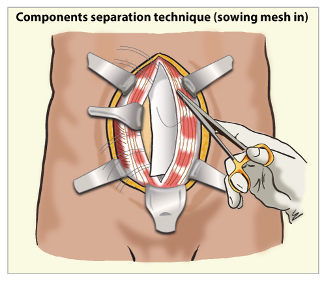
Patients needing abdominal wall reconstruction are those with large ventral hernias and excess skin and fat mainly below the belly button. Certain patients with a midline abdominal hernia may benefit greatly by the release of their rectus abdominis muscles (the muscles responsible for a 6-pack) from their side attachments to allow them to be shifted to the middle. This procedure known as a ‘components separation’ aims to restore the natural anatomy that has been obliterated as a result of the hernia. When combined with the placement of a mesh this technique provides a reliable long-term solution to this oftentimes debilitating condition. Plastic surgeons are uniquely well suited to performing this procedure, as their expertise is in the movement of bodily tissues, especially muscle, to treat a wide variety of possible defects.
What is an abdominoplasty/panniculectomy?
Abdominoplasty refers to removal of excess skin and tightening of abdominal muscles. Panniculectomy refers to the removal of pannus, which is an overgrowth of skin and adipose tissue that does not respond to traditional forms of weight loss. Combining removal of excessive skin and fat with tightening of midline abdominal muscles, gives patients a flatter and more cosmetically pleasing abdomen. These two procedures can be combined to the extent necessary to deliver the desired results and customized for each patient based on their underlying anatomy and ultimate cosmetic goal.
Surgery:
This surgical procedure can be performed in both an outpatient and inpatient setting depending on the patient’s need for surgery. Most commonly patients with abdominal wall hernias require a night in the hospital, to help with pain control. Those admitted for observation and pain control to the hospital will be rounded on daily while inpatient and will then follow up in our office 5-7 days after discharge.
Things to know:
- Patients will have approximately 2 drains after surgery. Inflammation from surgery causes an accumulation of serous fluid that is managed with these drains. You will need to milk and empty these drains, recording the output preferably twice daily and at the same time each day. Drains will remain in place until output is less than 30ml for an entire 24-hour period.
- You must wear an abdominal binder post operatively at all times, except when showering.
- You may begin showering in 48 hours after surgery. When showering, wash all areas with soap and water, and pat dry with a towel. It is important that you do not submerge your surgical incision in water (i.e. no bath tubs, swimming pools, etc.).
- Sutures will be absorbable. Follow up appointments will be scheduled on a weekly basis until drains are removed, at which time follow up appointment will typically be schedule in two-week intervals. You may begin scar massage and use of scar creams approximately 3 weeks after surgery.
Postoperative restrictions are as follows:
No heavy lifting, pushing, or performing any activities that engage the abdominal muscles for 6-8 weeks. We will gradually increase the weight you may lift and your activities over the next few weeks. At 8- 12 weeks you are cleared for full activity.